Background
In 2021, the Vermont Department of Health asked PDA to conduct a needs assessment to help inform the next Supplemental Nutrition Assistance Program Education (SNAP-Ed) three-year plan. The goal of SNAP-Ed is to improve healthy eating and physical activity behaviors among households with low incomes. The SNAP-Ed program pursues this goal through three types of evidence-based strategies: direct education, social marketing, and policy, systems, and environmental (PSE) changes. The Health Department wanted to know how to focus its efforts to promote health equity, but county-level data often masked more localized geographic disparities, and limited surveillance data were available for certain communities and populations, such as refugees and New Americans and Indigenous Abenaki communities.
Approach
The motivating question for the needs assessment was, “Which communities or populations should SNAP-Ed focus on reaching in order to reduce nutrition-related health inequities in the SNAP-eligible population?” To answer this question, demographic data, health statistics, and interview data were examined to identify communities and populations that were disproportionately likely to be eligible for SNAP and marginalized as a result of their race, ethnicity, place of birth, sexual orientation, gender identity, disability status, socioeconomic status, age, or geography. This list of factors was generated based on data availability and priorities set by the health department.
PDA compiled existing surveillance data from the 2020 Census, American Community Survey, Behavioral Risk Factor Surveillance System, and past state reports; created census-tract level maps showing the number and percent of households eligible for SNAP; conducted a targeted literature search; and interviewed four individuals who each worked with one specific marginalized population: Abenaki; refugees; Lesbian, Gay, Bisexual, Transgender, Queer/Questioning (LGBTQ+); and living with a disability. PDA then conducted a gap analysis in collaboration with health department staff to identify who was not being reached by the program and how program requirements and practices could be changed to better reach them.
Results
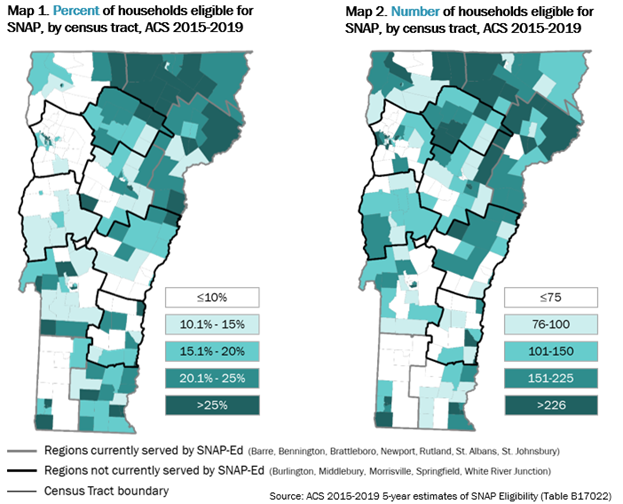
The program had previously restricted access to SNAP-Ed services to certain regions of the state, in an attempt to direct resources to the counties that were most in need. However, the maps below demonstrated that county-level data masked local-level differences in SNAP eligibility, meaning that restricting funds to certain regions of the state was neither an equitable nor effective way of reaching SNAP-eligible households.
Furthermore, the gap analysis revealed that services did not reach many Abenaki people or people of color, and no data were collected on the extent to which services reached refugees, LGBTQ+ people, and people with disabilities. Key informant interviews revealed structural barriers to high-quality data collection and programming with marginalized populations, such as historic and ongoing institutional mistreatment of Abenaki communities in Vermont that make many Abenaki individuals reluctant to identify as such on government forms; language and literacy barriers that make it difficult for refugees to understand and meet each program’s administrative demands; lack of cultural competence and tailoring for the unique situation of LGBTQ+ people; and structural barriers to obtaining healthy foods among adults with a disability, such as lower wages, restrictions within food benefit programs, transportation challenges, and physically inaccessible food access spaces.
As a result of the needs assessment, the health department changed the program requirements to allow implementing organizations to work in any part of the state and to prioritize partnerships (between implementing organizations and organizations working in and with the focus populations. The health department also asked PDA to develop an equity evaluation framework that implementing partners would use to evaluate their efforts to reach focus populations.
Related Highlights
Using principles-focused evaluation to embed health equity in an initiative
PDA engaged program staff and community partners in revising and assessing program principles that reflect health equity processes and outcomes.
Using principles-focused evaluation with a complex, multi-grantee initiative
PDA used a principles-focused evaluation framework to guide our evaluation of a statewide initiative to prevent chronic disease.
Facilitating learning for a health equity-focused community grant program
PDA's evaluation helped the Hawai'i Community Foundation share successes and opportunities in serving priority populations.
See More Highlights
Our Team
Our dedicated and talented team is united by our common desire to improve communities.

Heather Zook
Senior Evaluator II

Amy Kerr
Director of Evaluation

Belle Federman
Principal Researcher

Angie Ficek
Senior Evaluator II